
Subvastus Approach to Total Knee Replacement
When you hear the term “subvastus approach,” it can sound like a special type of knee replacement. It’s not.
The subvastus approach is simply how I get into the knee-not a different implant, not a different operation, and not a different “brand” of knee replacement.
Think of It Like a Door
Every knee replacement has the same goal:
- Remove damaged cartilage
- Resurface the joint
- Restore alignment, stability, and motion
The approach is just the door I use to get there.
Sometimes that door can be smaller and less disruptive. Other times it needs to be a bit larger. The key is that the door must be big enough to safely do the work on the other side. You wouldn’t try to move a large piece of furniture through a tiny doorway-and the same principle applies in surgery.
My philosophy is simple:
Use the least invasive approach possible-without ever compromising accuracy or safety.
Where the Subvastus Approach Fits
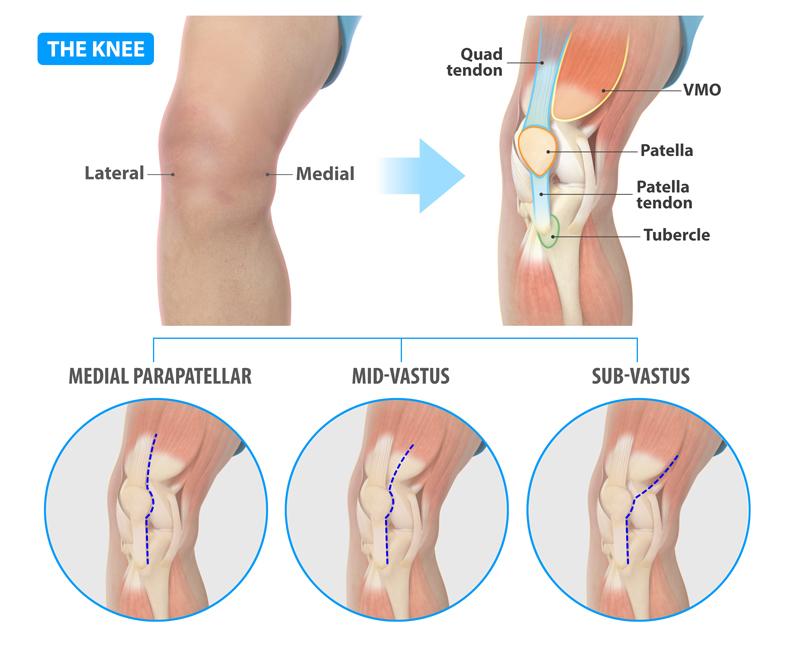
The subvastus approach goes under the quadriceps muscle (vastus medialis) instead of cutting through it. That means:
- No splitting of the quadriceps tendon
- Less direct muscle trauma
- Potentially smoother early recovery
In my practice, most patients can and do have a subvastus approach, and I’ve incorporated this into my knee replacement technique since 2022.
I’m genuinely proud to be able to offer this approach to my patients. When combined with multimodal anesthesia, modern alignment strategies, and precise implant placement, I’ve found it to be a helpful adjunct in improving early recovery and patient experience.
What the Research Shows
This isn’t a new idea-it’s an approach that’s been around for decades. What’s changed is our focus on early recovery and minimizing tissue disruption.
Studies comparing subvastus to more traditional approaches generally show:
- Less pain and improved early function (especially in the first ~4–6 weeks)
- Earlier return of quadriceps strength and straight-leg raise
- Similar outcomes by 3–6 months and beyond
In other words:
It may help you feel better sooner, but long-term results are similar regardless of approach.
It’s One Piece of the Puzzle
The approach is just one variable I consider when planning your surgery, along with:
- Implant design and shape
- Alignment strategy (kinematic, functional, mechanical)
- Use of technology, including robotic assistance
A subvastus approach can be performed with or without robotic assistance.
Other sections of this site go into detail on each of these topics so you can understand how they all work together.
Not One-Size-Fits-All
While I use the subvastus approach in most patients, it’s not always the best choice.
- If there is severe patellar (kneecap) arthritis, I may use a small midvastus approach to ensure I can properly access and resurface the patella.
- In revision surgeries or certain prior incisions, a different approach may be safer.
- If exposure becomes too limited, forcing a “small door” can actually increase risk
There are also some tradeoffs:
- Access to the patella can be more challenging
- If the dissection extends too far upward, there can be more bruising or bleeding due to small blood vessels in that area
The Bottom Line
The subvastus approach is not a different knee replacement—it’s simply a way to access the knee.
- It allows for a muscle-sparing pathway that can improve early recovery in many patients
- The best approach is individualized based on your anatomy and surgical needs
My goal is always the same “Do the operation safely, place the implants precisely, and give you the best possible outcome” using the least traumatic path to get there.





