
Your Total Knee Replacement: Understanding the Subvastus Surgical Approach
What Is Total Knee Replacement?
Total knee replacement (also called total knee arthroplasty, or TKA) is a surgical procedure in which the damaged surfaces of the knee joint are replaced with metal and plastic implant components. It is one of the most successful operations in all of medicine, with the vast majority of patients experiencing significant pain relief and improved function that lasts for decades.
To perform this surgery, I must make an incision in the skin and then open the deeper tissues around the knee to access the joint. The way I enter the joint - called the “surgical approach” - can vary. The approach chosen affects how the muscles and soft tissues around the knee are handled during surgery, which can influence your early recovery.
The Main Surgical Approaches to the Knee
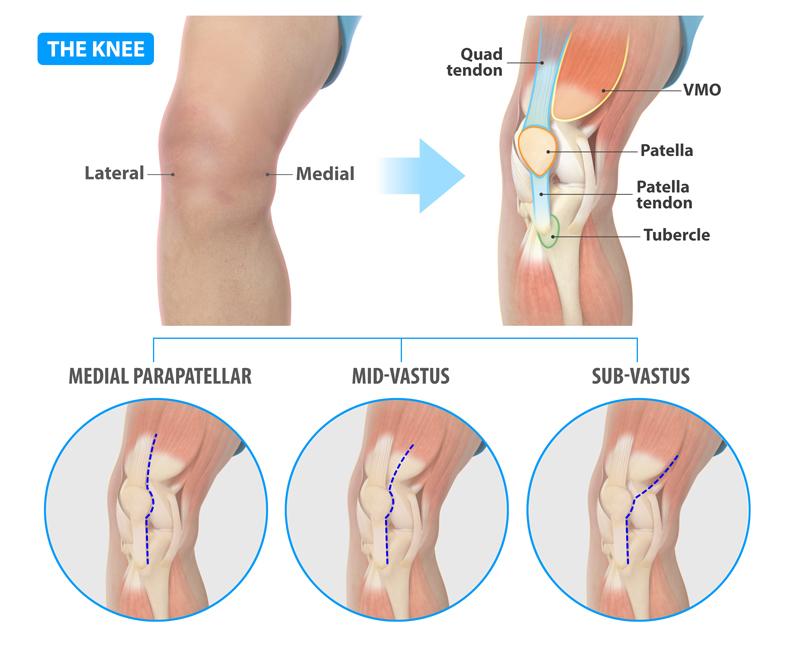
There are three common approaches used to access the knee joint during a total knee replacement. All three use a similar skin incision on the front of the knee - the key difference is how I work through the deeper muscle and tissue layers beneath the skin.
- Medial Parapatellar Approach: This is the most commonly used approach worldwide. The surgeon makes an incision through the quadriceps tendon (the large tendon just above the kneecap) to enter the joint. It provides excellent visibility and access to the joint, making it very versatile. However, because it cuts through the quadriceps tendon, it can temporarily weaken the thigh muscle and may cause more pain in the early days after surgery.
- Subvastus Approach: Instead of cutting through the quadriceps tendon, I enter the joint by going underneath the vastus medialis muscle (the teardrop-shaped muscle on the inner side of the thigh, just above the kneecap). The muscle is lifted up rather than cut. This preserves the entire quadriceps mechanism - the muscle, tendon, and their connection to the kneecap remain completely intact.
- Mid-Vastus Approach: This is a “middle ground” between the two approaches above. I make a short split through the muscle fibers of the vastus medialis rather than going completely underneath it or cutting through the tendon above it. It provides more exposure than the subvastus approach while still causing less muscle disruption than the standard parapatellar approach.
Why I Prefer the Subvastus Approach
In my practice, the subvastus approach is my routine approach for primary total knee replacement. The reason is straightforward: by preserving the quadriceps mechanism entirely, this approach offers meaningful advantages during the early recovery period - the time when patients are working hardest to regain mobility and independence.
Research involving thousands of patients across dozens of clinical studies has consistently shown that the subvastus approach provides:
- Less pain in the first days and weeks after surgery. Because the quadriceps muscle and tendon are not cut, there is less tissue trauma. Studies show significantly lower pain scores in the first 1–7 days compared to the standard parapatellar approach.
- Faster return of knee motion. Patients treated with the subvastus approach tend to bend their knee more easily and more quickly in the early postoperative period. Some studies show a range-of-motion advantage that persists up to 6 months after surgery.
- Earlier ability to perform a straight leg raise. Lifting the leg straight off the bed is one of the first milestones after knee replacement. Because the quadriceps muscle is intact, patients can often achieve this sooner - sometimes a full day earlier than with the standard approach.
- Faster overall functional recovery. Patients may walk independently sooner, negotiate stairs earlier, and leave the hospital sooner. One study showed patients in the subvastus group were weight-bearing without assistance nearly a full day earlier and had a shorter hospital stay.
- Less blood loss during surgery. Multiple studies have found that the subvastus approach is associated with reduced surgical blood loss compared to the standard approach.
It is important to understand that these advantages are most noticeable in the first days to weeks after surgery. By 3–6 months, and certainly by one year, patients who had any of the three approaches tend to have very similar outcomes in terms of pain, function, and satisfaction. The subvastus approach does not change the final result - it helps you get there faster and more comfortably.
Are There Any Disadvantages to the Subvastus Approach?
Like any surgical technique, the subvastus approach has some trade-offs:
- More limited surgical exposure. Because I am working underneath the muscle rather than through it, the “window” into the joint is somewhat smaller. This requires more surgical skill and experience to ensure the implant components are positioned accurately. In the hands of an experienced surgeon, studies have shown that implant positioning is equivalent between approaches.
- Slightly longer operative time. Some studies report that the subvastus approach takes a few minutes longer than the standard approach. This difference is generally small and does not affect outcomes.
- Not suitable for every patient. In certain situations, the subvastus approach may not provide enough room to safely and accurately perform the surgery. These situations include:
- Patients with a low-riding kneecap (a condition called patella baja or patella infera), which makes it difficult to work underneath the muscle
- Revision surgery (replacing a previously implanted knee replacement), which requires more extensive exposure
- Patients with very stiff knees, significant deformity, or very muscular or large thighs
- Patients who have had a prior surgical approach in the same area that may have altered the tissue planes
When I Use the Mid-Vastus Approach Instead
In cases where the subvastus approach may not provide adequate exposure - such as patella baja, revision surgery, or when a prior subvastus approach has been performed - I may use the mid-vastus approach as an alternative.
The mid-vastus approach is best thought of as existing on a spectrum:
- At one end, it can be performed very similarly to a subvastus approach, with only a very short split in the muscle fibers - preserving most of the quadriceps mechanism.
- At the other end, the muscle split can be extended further, providing exposure that approaches what the standard parapatellar approach offers.
This flexibility is one of the mid-vastus approach’s greatest strengths. I can tailor the amount of muscle splitting to the specific needs of each case - using the minimum amount necessary to achieve safe, accurate implant positioning. Like the subvastus approach, the mid-vastus approach has been shown to offer some early recovery advantages over the standard parapatellar approach, including less pain and better early range of motion. A large national registry study of over 875,000 knee replacements found that the mid-vastus approach was associated with a 20% lower risk of revision surgery compared to the standard parapatellar approach.
Dr. Gilmer’s Philosophy: Minimally Invasive When Possible, Never at the Expense of Accuracy
My guiding principle is simple:
I routinely use the most minimally invasive approach available - the subvastus approach - because it provides better short-term recovery for my patients. Less pain, faster motion, quicker return to independence.
However, I will never compromise surgical exposure when it is needed to achieve the best possible implant positioning. Accurate implant positioning is what determines the long-term success of your knee replacement - how well it functions, how natural it feels, and how long it lasts. Research has clearly shown that component alignment in all planes (front-to-back, side-to-side, and rotation) plays a significant role in implant survival and long-term function.
In the small number of cases where the subvastus approach does not provide adequate exposure, I transition to a mid-vastus approach - and I adjust the extent of that approach as needed for each individual patient. The goal is always the same: the best possible implant positioning with the least possible tissue disruption.
This balanced philosophy means that every patient receives an approach tailored to their specific anatomy and surgical needs, optimizing both short-term recovery and long-term success.
What This Means for You
- In most cases, your surgery will be performed using the subvastus approach, and you can expect the recovery benefits described above.
- If I determine during your preoperative evaluation - or during surgery itself - that a different approach is needed for safe and accurate implant placement, I will use a mid-vastus approach instead.
- Regardless of which approach is used, the implant, the anesthesia, the pain management plan, and the rehabilitation protocol will be the same. The long-term outcome of your knee replacement is expected to be excellent with either approach.
- I will discuss the planned approach with you before surgery and will explain if any factors in your case may require a different technique.
If you have any questions about the surgical approach planned for your knee replacement, please do not hesitate to ask during your preoperative visit with Dr. Gilmer.
| Approach | Incision/Dissection | Effect on Extensor Mechanism | Exposure Quality | Advantages | Disadvantages / Contraindications | Typical Joint Exposure |
|---|---|---|---|---|---|---|
| Medial Parapatellar | Midline skin incision + arthrotomy through quadriceps tendon (medial to patella), extending into vastus medialis insertion | Disrupts quad tendon partially; patella everted laterally | Excellent, even in difficult cases (obese, stiff knees, deformity) | Familiar, highly extensile, great visualization | May impair patellar blood supply, slower quad recovery, risk of patellar maltracking | Full eversion of patella; wide open joint |
| Midvastus | Similar skin incision; split through vastus medialis (VMO) muscle fibers (usually 2–4 cm proximal to patella), spares quad tendon insertion | Preserves quad tendon; partial VMO split | Good (slightly less than parapatellar) | Faster early recovery, better patellar tracking, less disruption | Less extensile; harder in obese/stiff knees or limited ROM | Patella subluxed (not always fully everted) |
| Subvastus | Midline skin incision; lift entire VMO off intermuscular septum without cutting muscle or quad tendon | Fully preserves extensor mechanism and VMO insertion | Adequate for straightforward cases | Best early quad function, preserves patellar vascularity, minimal lateral release needed | Least extensile; challenging in obese, muscular, or deformed knees | Patella subluxed laterally; joint accessed by mobilizing VMO upward |





